Introduction–Ergonomics & Computer Injuries FAQ
Jonathan Bailin, Ph.D. © 2014
FACTS: Repetitive Strain Injuries (RSI’s) such as Carpal Tunnel Syndrome increased 10 fold from 1983 to 1993 as computer use skyrocketed. In 1994, the US Bureau of Labor Statistics wrote that, “RSI disabled over 300,000 for a cost of between $20-100 billion a year”. It is safe to say that today, because of even more screen use, costs are greater.
Even back in 1993, OSHA concluded that carpal tunnel injures lead to more lost work time than amputations or fractures. Ever since, RSI’s have remained the most common injury in the workplace.
Don’t let your keyboard, tablet, or phone screen make a statistic out of you! My name is Dr. Jonathan Bailin. You can read more about me later. This document was originally created by my moderated newsgroup (misc.health.injuries.rsi.moderated) on the Internet from 1995-2000 but the information in it now more precious than it has ever been for millions and millions of screen users. It was a cooperative effort between the USC Medical School and the USC College of Letters Arts & Sciences.
The newsgroup provided expert opinions about Repetitive Strain Injuries (RSI’s) from a variety of medical experts at the USC University Hospital, and me the moderator, who formed our panel. As the previous facts point out, most RSI’s are due to keyboard/mouse/screen use, though many come from blue collar jobs like construction, plumbing, and manufacturing. Oddly enough, many politicians during political campaigns get it from shaking hands. Hundreds, if not thousands, of hand shakes a day!
The FAQ below was designed to focus discussion and respond to many, if not most, computer use health questions. It has been used internationally at Exxon in Malaysia, Microscopy Today, Better Health and Medical Network, Canadian Centre for Occupational Health and Safety, Law Offices of Sydley & Austin, the Dallas Community Colleges, Institut fuer Medienkommunikation–Germany, North Carolina State University, Centro de Investigaciones Biologicas del Noroeste– Mexico, National Association of Legal Secretaries, Leeds University (England), Belgium Journalists Bureau, Microsoft Corporation, MIT, NASA, and the US Food & Drug Administration.
Please do not reproduce this FAQ without consulting me at ErgonomicsDr@gmail.com You may not change the content of the FAQ in any way but you may reformat it to better integrate it with your production media.
For those of you new to RSI pain, don’t minimize its threat. It is a serious, and frequently career threatening, affliction. Your early attention to it is usually critical. To conquer it, prepare to make behavioral and lifestyle changes as no best piece of equipment, technology, or magic bullet exists.
You should also know that new laser treatments are showing great promise for those diagnosed with all forms of tendinitis. Another new source of help is the book, “The Truth About Carpal Tunnel Syndrome: Finding Answers, Getting Well”, by Jill Gambaro (Rowman & Littlefield).
The more informed you are about RSI, the lower your risk of disabling injury, and the stronger your “healing partnership” with your attending health care practitioner will be. That’s why the original newsgroup was conceived. Prevention along these lines will remain the best cure. I want to wish all of you the best of luck in stopping RSI.
Sincerely,
Jonathan Bailin, Ph.D.—Former Moderator
misc.health.injuries.rsi.moderated
Ergonomics & Computer Injury: FAQs
Jonathan Bailin, Ph.D.
Exercise Physiology/Ergonomics/Biomechanics
Sports Medicine & Ergonomics Associates ErgonomicsDr@gmail.com
About the Author–
During doctoral research in Exercise Physiology/Biomechanics at the University of Southern California, Jonathan completed ground breaking electromyographic (EMG) research on repetitive strain injuries (RSI) to the forearm. In 1995, he created the first, free internet medical service dedicated to helping with RSI and wrote this orientation document which is now used around the world. Over the last 10 years, Jonathan has produced seminars, articles, and dialog on sports medicine and ergonomics topics while consulting for Los Angeles firms.
FAQ QUESTION INDEX
General Info, Component Position, & Desktop Accessories….Q1-6
Wrists, Body Posture, & Chair Features…………………………Q7-13
Active Breaks, Microbreaks, & Exercises………………………Q14-15
Varieties of Computer Injuries………………………………………Q16
Kinesiology for RSI…………………………………………………….Q17
Emergence and Politics of RSI………………………………………Q18-19
Lifestyle Changes and Reducing RSI Risk………………………Q20
Speech/Voice Recognition Software………………………………..Q21
EMG/NCV Test Reliability…………………………………………….Q22
Expert Panel Members…………………………………………………..Q23
New Laser Treatments……………………………………………………Q24
1) Q. What is “ergonomics”?
A. Ergonomics is the science of adjusting your work environment to fit your body and make it most comfortable.
2) Q. What is the best room lighting to help reduce eye strain?
A. A mixture of fluorescent and incandescent light is usually most pleasing. The most important aspect of lighting is to reduce glare and bright reflections from your screen, nearby glass, or shiny surfaces. Since light conditions change during the day this may require several adjustments while working. If you smoke while keyboarding, be sure to clean your screen frequently, as water vapor and smoke form a potent film.
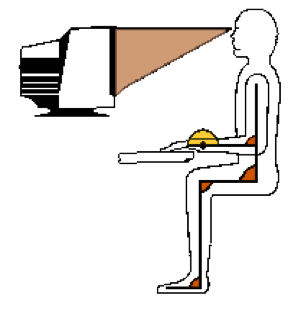
3) Q. What is the best position for the monitor at my workstation?
A. Many make the mistake of putting the monitor, the keyboard, or both off to one side of their desk. If you perform more than a few minutes of keyboarding a day, the keyboard and monitor should be placed directly in front of your normal sitting position. The screen should be 18-30 inches from your eyes, or about an arm’s length.
4) Q. Is there an optimum height for my monitor and mouse?
A. Yes. The top of the monitor should be at eye level because the eyes are at their most comfortable position straight ahead but slightly downward. This is why reading lenses in bifocal glasses are placed just below the horizontal plane. This posture also makes it easiest to balance your head above your shoulders with the least muscular effort.
On the topic of eye correction, make sure your eyes have been examined recently and that if you do need correction your optometrist should know about the amount of your monitor use and its distance from your eyes. A correction just for monitor use may be necessary. Be sure to look away from your screen at least every 30 minutes and focus on something over 20 feet away.
Poor mouse operations can create RSI. At many work stations it is common to see the keyboard in proper position just above the knees, but the mouse is on a higher and more forward countertop. Mouse position should be on the same level as the keyboard so that mouse use does not create a twisted or reaching posture. A keyboard tray with a mouse shelf extension is one easy and inexpensive solution to this problem.
5) Q. Is there an optimum screen brightness and color scheme to help prevent eye strain?
A. Black characters against a light gray background are often easiest on the eyes for long periods. It is suggested that contrast and brightness should be adjusted to create the brightest screen without blurring.
6) Q. What other accessories and placements are important?
A. Frequently used items should be within arm’s reach from your keyboarding position. A document holder should be at the same height and distance as the screen so that your eyes don’t need to change focus frequently. Frequent telephone use *requires* a headset to avoid bending the neck while keyboarding. Remember that many RSI’s begin with nerve insult in the neck and shoulders.
7) Q. What is the most healthy posture for my wrists while typing?
A. The best position is neutral. In other words, the knuckles, wrist, and top of the forearm should form a straight line.
8) Q. Can a wrist pad sitting in front of the keyboard be used during keyboarding?
A. The neutral position described in #7 can not be achieved while in contact with most commercial wrist pads. For this reason keyboarding is best performed from a “floating” wrist position. Thus contact with wrist pads is best between bouts of keying only.
Frequent rest, away from the keyboard, becomes necessary with floating wrists because it tends to emphasize shoulder muscle contraction. Don’t forget to use the lightest possible finger pressure during keying.
9) Q. What is the best elbow and shoulder position while keyboarding?
A. The elbows should form a 90 degree angle while *hanging* at your sides from the shoulders. Rarely do chairs with armrests allow this position. It is *very* important that the shoulders remain relaxed in a lowered position during keyboarding (see #6).
10) Q. What is the best seat height for keyboarding?
A. It is most important that seat height should allow the upper body postures described in #7, #8, and #9. This upper body posture is most responsible for reducing risk of injury. Once this is accomplished, the feet should be flat on the floor.
If the resulting seat height prevents the feet from resting flat on the floor, a foot rest is necessary. Even a phone book can serve as an inexpensive solution. This should allow the lower legs to be vertical and thighs horizontal.
11) Q. What features should I look for in the backrest of a chair?
A. Expensive motors and adjustable sections are not necessary if the backrest has firm support for the inward curve of the lower spine (lumbar) and outward curve of the upper spine (thoracic). Whether you need upper body support to help keep your torso and head vertical is a matter of preference.
12) Q. What other characteristics of a chair are important?
A. The seat of the chair should be large enough to accommodate frequent changes in position and firm enough to allow your weight to be supported through the buttocks not the thighs. If others will use your chair, easy height adjustment is a must.
13) Q. How often should I change positions and take breaks during keyboarding?
A. You should change your sitting position at least every 15 minutes.
Active breaks should be taken at least every 30 minutes especially for those who perform more than 2 or 3 hours of keyboarding a day. Microbreaks should occur more often.
14) Q. What is an “active break” and a “microbreak”?
A. An active break occurs when you stop keyboarding to do other things, like take phone calls, file papers, or get up to get a drink of water. An active break should also include specific exercises. These exercises can also be performed during keyboarding microbreaks which occur while seated at your workstation.
15) Q. What are some of the best exercises for keyboarding microbreaks while seated?
A. The best exercises depend on your body’s vulnerable areas and/or your particular form of RSI, but here are a few favorites: the “Shoulder Blade Squeeze” is performed by raising your forearms and pointing your hands to the ceiling. Push your arms back, squeezing your shoulder blades together. Hold for at least 5 seconds and repeat 3 times.
“Eye Palming” is performed by placing your elbows on your desk, cup your hands, close your eyes, and place your eyelids gently down onto your palms. Hold this position for 1 minute while breathing deeply and slowly. Then uncover your eyes slowly.
The “Arm and Shoulder Shake”–drop your hands to your sides then shake your relaxed hands, arms, and shoulders gently for at least 5 seconds and repeat 3 times.
“Spanning”–place you arms straight in front of you and spread your fingers as far as possible for at least 5 seconds and repeat 5 times. Career pianists made this exercise famous. With the arms extended in front of you, spanning can be combined with a “Forearm Extensor Stretch”, by turning the hands so that their backs touch then, turning them so that the palms face the ceiling (“Forearm Flexor Stretch”).
These are only a few key exercises. Many more are useful for preventing repetitive strain. Try to find the best series for your areas of tension and particular relaxation needs.
**Frequent breaks yield better long term productivity!**
16) Q. I’ve heard many names for keyboard injuries. What do they all mean?
A. Repetitive Strain Injury (RSI) is a description of a manual injury associated with any repetitive activity such as hammering, piano playing, truck driving, computer use, or even shaking hands. Occupational Overuse Syndrome (OOS), Cumulative Trauma Disorder (CTD), and Work Related Upper Limb Disorders (WRULD), are all equivalent expressions to RSI.
Tendonitis and Tenosynovitis are characterized by inflammation of tendons or their surrounding sheaths, respectively. Both of these RSI disorders usually begin as mildly aggravating and, given bad habits, may quickly progress to be severely debilitating. These common RSI injuries also add to the difficulty of proper diagnosis and deserve greater recognition. These tendon inflammations usually occur before full blown Carpal Tunnel Syndrome (CTS).
Carpal Tunnel Syndrome is a specific, severe, and debilitating form of RSI which describes a squeezing of the median nerve as it runs into the hand. The nerve is squeezed by swollen tendons surrounding it as they cross through a bony passage (Carpal Tunnel) at the inside of the wrist.
The National Center for Health Statistics estimates at least 1.89 million people have Carpal Tunnel Syndrome. Many experts feel that CTS is also associated with nerve compression symptoms in the chest or shoulders.
**All RSI symptoms should receive immediate medical attention from physicians experienced in RSI. If you are not sure of their experience, ask!**
17) Q. Advice by Health Care Practitioners often includes a collection of terms from a kinesiology course. Which ones do I need to know to help identify my own workstation ergonomic problems?
A. Standing with the arms at your sides, palms facing forward, “flexion” is the folding of any joint of the body so that the angle between the parts decreases in the forward direction, except at the knee and toes. Returning the joint to its straight position requires “extension”.
A joint which continues its extension past it’s straight posture is in “hyperextension”. This occurs in the hand and wrist when you pull the fingers back.
Standing with your arms at your sides, palms facing forward, “pronation” is the turning of your hand so that your thumb points toward your leg. “Supination” is the opposite movement.
18) Q. Why does it seem like RSI from keyboarding has become such a big problem recently?
A. The reasons for recent increase in computer injuries are many. One major reason is that computers are now allowing us to do more office tasks which formerly allowed us to change activity or take breaks. For example, a typewriter at one time required using a return carriage, “white out” for mistakes, breaks for paper installation, and getting up to file papers in a cabinet.
Computer word-processing now eliminates these “microbreaks”. In short, computers have greatly simplified office activity, an advance that has at least one important disadvantage. The danger is found in the possibility for relatively motion free, long duration, continuous, and precise muscular activity called “static exertion”. Humans are not well “designed” for this. Defining high risk groups within the keyboarding population may explain other reasons for increasing RSI incidence.
19) Q. What groups are likely to experience higher incidence of RSI?
A. Undoubtedly, women still hold the majority of keyboarding jobs since the computer revolution. Unfortunately, most of their chairs, tables, and other ergonomically important accessories are scaled to antiquated male proportions. More importantly, regardless of the worker’s gender, even the most healthy work habits can be overcome by poor ergonomics.
The quality of workstation ergonomics is also inevitably linked to office economics. For example, departments on tight budgets are less likely to provide proper computer workstation furniture, less likely to control workload dynamics and crises deadlines, and less likely to appreciate reports of dangerous working conditions and RSI injuries. Assuming that women disproportionally hold lower paid, high production, high stress jobs with less work flow control, it would be no surprise that gender is a significant variable in the RSI incidence formula.
Long-standing issues of discrimination against women in the workplace and health care industry gain extra spin when added to the RSI equation. With recognition of RSI’s in the United States still in its infancy, gender slurs that RSI occurrence in women is predominantly hormone based hysteria or more native to “weaker” physiology abound. In contrast, even informal reports from health care providers testify to the dominance of behavioral and ergonomic factors in RSI etiology.
Among men, treatment reports reveal that a preponderance of injuries occur among those with smaller builds who are also mismatched with furniture provided for computer operations. Health care professionals often point to two of the most “popular” sites of high production/high stress within the graphic arts and legal word processing fields. These departments commonly experience long breakless work sessions, cast-off chairs and tables, and relentless deadlines. Just imagine if such sessions were performed on laptops!
As in the rest of the work sector, the threat of retaliation is more likely to fall on those most desperate for employment. Retaliation, including firing, is one of many important factors reviewed here which makes study of RSI epidemiology difficult. If you are a caring citizen, you now have more than enough reason to demand more robust OSHA policies and budgets from your representatives.
20) Q. What lifestyle changes can I make to reduce the chances of RSI?
A. Two main themes permeate ergonomic study of RSI prevention: posture and relaxation. Appropriate posture is necessary to keep the strain of performing work in a near stationary position (static exertion) to a minimum. But even the best posture can fall prey to overload when combined with bad work habits.
Relaxation is critical to the body’s resilience, its ability to recover from keyboarding. Office workload dynamics, both good and bad, can have a great influence on the occurrence of RSI. Try to promote office policies, which emphasize steady work load schedules and avoid, or at least distribute, crises deadlines.
Over the last few years voice recognition has become a realistic and affordable accommodation which employers should be asked to consider. The alternative of losing a good employee, far outweighs the relatively low cost for these upgrades. Now back to your body…
Stretching and strengthening active muscles promotes relaxation. Relaxation is as important for prevention of RSI symptoms as it is for general well-being. Take a new, more active role in promoting your general fitness both at and away from work. If you don’t exercise regularly and your over 40, get clearance from a physician to add walking, bicycling, or swimming to your weekly schedule on three separate days.
Cut down on stimulants like coffee, sweets, or nicotine and spread healthy snacks and water intake throughout the day. Keep water at your desk as it makes for a smart microbreak. Remember, the first symptom of dehydration is fatigue, not thirst!
Fruit and vegetable snacks prevent mid-morning and mid-afternoon blood sugar drops. These dips can effect alertness, mood, productivity, and decision making. A diet emphasizing complex carbohydrates, reliable sleeping patterns, and time for yourself can do wonders for 9 to 5 productivity, not to mention your own well-being. All habits and practices that promote relaxation and physical fitness are potent weapons to stop the threat of RSI. Good Luck.
21) Q. Some say that Speech Recognition (SR) software is the perfect answer to RSI, but others say there is great danger of voice injury. What is the RSI Panel’s current position?
A. The RSI Panel currently has no credentialed specialist in this field but we
still felt it necessary to forward an educated opinion on the potential dangers of voice overuse which may accompany SR use. We therefore solicited a professional opinion from a Speech Language Pathologist (SLP) who is certified by the American Speech Hearing Association (ASHA). The following is a reprint of that opinion:
“Using Voice Recognition (VR) or Speech-Recognition (SR) software for long periods of time should not cause damage to your vocal folds if you’re
relaxed, drink lots of non-caffeinated fluids, take breaks, and use sufficient breath support. It’s not how long you talk, it’s *how* you talk.”
“If you experience any hoarseness or discomfort after using VR software, your best option is to consult an SLP with expertise in voice disorders. To find
one, ask a local Otolaryngologist, or Ear/Nose/Throat (ENT) specialist. Most ENT’s work with or know SLP’s who are appropriate for your needs.”
“An SLP can train you to breathe and speak properly in order to minimize
vocal stress and help avoid discomfort or injury to your vocal folds. Its likely that an SLP will refer to an ENT for medical screening even before starting treatment.”
“Voice coaches can also help those suffering from vocal strain, but they
may lack the background to know when to refer clients to a medical specialist. This distinction may be critical as voice problems can be caused by serious medical conditions such as allergies, polyps, tumors, etc.”
The RSI Panel has noticed that SR software has come a long way recently.
Our readers should know that two important improvements rank above the rest.
Formerly, SR software was “discreet” in that each word had to be separated by a pause. Now the new software is “continuous” which is of course more like natural speech.
The second great change is in price. Most SR software is now $200 or less, a price that should tempt anyone who wants to reduce keyboarding time. But it is still not a panacea.
Training and correction time can be considerable and disillusioning. According to Consumer Reports (Nov ’98) don’t count on saving time if you type faster than 30 words a minute or just want to create a single page document. Still, for the majority of serious RSI sufferers, speech recognition software can be a godsend.
22) Q. To confirm Carpal Tunnel Syndrome (CTS), experts place a lot of emphasis on Electromyographic (EMG) and Nerve Conduction Velocity (NCV) tests. How diagnostic are these tests?
In the hands of a skilled expert, EMG’s and NCV’s can provide a great deal of useful information about the health of your nerve tissue. Besides helping in the diagnosis of CTS these studies can diagnose other diseases and injuries and track the progress of healing. Again these tests are not perfect and require skilled interpretation.
About 20% of patients with CTS have negative EMG/NCV tests. In order to have electrical changes in the nerve during these tests, the nerve must be continuously compressed for at least a couple of weeks depending on the pressures involved. Thus if your nerve is compressed intermittently by day to day changes in the swelling, you may never have a positive study. This does not mean that you DO NOT have symptomatic CTS that may require surgical or non-surgical treatment, as the intermittent compression can be just as troublesome as the continuous form.
So a negative study is not conclusive of the absence of CTS.
In summary, EMG/NCV tests are only a piece of the CTS puzzle. For an experienced RSI diagnostic physician, symptoms and history can often be sufficient to properly diagnose true CTS.
23) Q. Who were the other expert panel members?
A. (in existence from 1995-2000)
UNIVERSITY OF SOUTHERN CALIFORNIA MEDICAL ADVISORY PANEL ON RSI
Jonathan Bailin, Ph.D.–Sports Medicine & Ergonomics (Moderator)
Najmedin Meshkati, Ph.D.–Ergonomics
Sharon K Lee., O.T.R., C.H.T.–Director, The Hand Rehabilitation Center
Garry S. Brody, M.D.–Medical Director, USC Hand Rehabilitation Center
Stephen B. Schnall, M.D.–Chief of Hand Surgery USC Medical Center
Joan F. Wright, M.D.–Hand Surgery, Plastic Surgery, RSIs
John Shen, M.D.–Physical Medicine/Diagnostics
Mary Hume-Neal, M.D.–Spinal Disorders/Surgery
Michael Patzakis, M.D.–Osteomyelitis and Joint Infections
Thomas Vangsness, Jr., M.D.–Disorders/Surgery of the Knees & Shoulders
Najmedin “Naj” Meshkati, Ph.D.–Ergonomics
Dr. Meshkati is Professor of Human Factors and Ergonomics, the Associate Executive Director for Professional Programs at the Institute of Safety and Systems Management, and teaches at the Department of Industrial and Systems Engineering at USC. Dr. Meshkati is a Certified Professional Ergonomist (CPE # 650) and is a member of the Review Panel for the National Research Council (NRC), which is the principal operating agency of the National Academy of Sciences and the National Academy of Engineering.
Dr. Meshkati has consulted for such organizations as: Aerospace Corporation, ARCO, Aviotex Corporation, Jet Propulsion Laboratory, Orange County Transit District, Perceptronics Inc., Pneumo Abex Corporation, Rockwell International, Semiconductor Equipment and Materials International, United Parcel Service, the United Nations Industrial Development Organization, and the US Navy. He is also in the International Atomic Energy Agency’s Coordinated Research Program on Human Error Classification and Data Collection.
Sharon K Lee., O.T.R., C.H.T.–Director, The Hand Rehabilitation Center, USC University Hospital
Ms. Lee, is a registered occupational therapist and certified hand therapist with more than 10 years of hand rehabilitation experience. In 1991, she was among the first group of therapists to take and successfully complete the exam to become a
certified hand therapist. Her clinical experience, combined with her administrative skills, gives her unique insight into managing a sophisticated Hand Rehabilitation Center. She is a clinical instructor of Occupational Therapy at USC.
Garry S. Brody, M.D.–MEDICAL
Dr. Brody founded and directed the first comprehensive hand rehabilitation center in California in the city of Downey 20 years ago. He is past president of the American Association for Hand Surgery and is a professor of plastic surgery at USC. As Medical Director of the Hand Rehabilitation Center, Dr. Brody oversees the medical components of the program. He is currently president-elect of the American Society of Plastic and Reconstructive Surgery. Dr. Brody’s special interests include chronic trauma and upper extremity pain syndromes.
Stephen B. Schnall, M.D.–MEDICAL
Dr. Schnall serves as Assistant Professor of Orthopaedic Surgery and Chief of Hand Surgery at Los Angeles County and USC Medical Centers. He is a Joseph H. Boyes Hand Fellow and directs this program at USC which is the oldest formal fellowship for surgery of the hand in the United States. In 1990, Dr. Schnall earned the Certificate of Added Qualifications in Surgery of the Hand. He is also a Fellow of the American Academy of Orthopaedic Surgery and the American Society for Surgery of the Hand.
Joan F. Wright, M.D.–MEDICAL
Dr. Wright is an Assistant Professor of Clinical Surgery (Plastic and Reconstructive) at USC University Medical Center with a Certificate of Added Qualifications in Surgery of the Hand. She has a special interest in cumulative trauma disorders (CTD’s) or repetitive trauma disorders linked to repetitive activities and/or vibrating tools. Dr. Wright is a member of the American Society for Surgery of the Hand, American College of Surgeons,
and Association of Women Surgeons.
John Shen, M.D.–MEDICAL
Dr. Shen is an Assistant Professor of Orthopaedic Surgery at the USC University Medical Center’s Department of Orthopedics and the Department of Physical Medicine and Rehabilitation. He is the Medical Center’s leading specialist in performing electromyographic and neural conduction tests for RSIs as he is Board Certified by the American Board of Physical Medicine and Rehabilitation and the American Board of Electrodiagnostic Medicine.
Mary Hume-Neal, M.D.–MEDICAL
Dr. Hume-Neal is an Assistant Professor of Orthopaedic Surgery in the Department of Orthopedics at the USC University Medical Center. She is Chief of the Orthopaedic Spine Service at the Los Angeles County and USC University Hospital Medical Centers and is Director of the Orthopaedic Spine Center at the University Hospital. She has held spinal surgery fellowships in Sweden, Switzerland, and the US. She is a Board Certified Diplomate by the American Board of Orthopaedic Surgery.
Michael Patzakis, M.D.–MEDICAL
Dr. Patzakis is Professor and Chairman of the Department of Orthopedics at USC’s School of Medicine. He is Chief of the Orthopaedic Infection Service with special interests in joint infections and infected non-unions at the LA County and USC Medical Centers. He is Board Certified by the American Board of Orthopaedic Surgery.
Thomas Vangsness, Jr., M.D.–MEDICAL
Dr. Vangsness is Associate Professor of Orthopedics, Department of Orthopedics at the USC School of Medicine. He performed a Sports Medicine Fellowship at the Kerlan-Jobe Orthopaedic Clinic in Inglewood, California. He is Board Certified by the American Board of Orthopedic Surgery.
24) Q. Are there any promising treatments for RSI or CTS being used today?
A. Yes! Laser treatments have proved to be extremely effective for many forms of soft tissue injury including all forms of tendinitis such as Plantar Fasciitis, Tennis Elbow, and Carpal Tunnel Syndrome.
This FAQ is copyright (C) 2014 by Jonathan Bailin, Ph.D.